


Core IM: 5 Pearls on Contrast-Induced Nephropathy
Update: 2018-05-16
Description
By Daniel Sartori MD, Marty Fried MD, Shreya Trivedi MD; Illustration by Michelle Lo MD and Amy Ou MD. Quiz yourself on the 5 Pearls we will be covering:
* Are there diagnostic criteria for contrast-induced nephropathy (CIN)? (2:11 )
* Is there a difference between exposure to intra-arterial versus intra-venous contrast in terms of risk of CIN? (6:28 )
* What are the biggest risk factors for CIN? (14:48 )
* What preventive measures have been shown to best reduce the risk of CIN? (19:41 )
* Can ESRD patients on hemodialysis still suffer from CIN? (23:32 )
* Recap (25:49 )
A special thank you to Dr. Josh Farkas for peer-reviewing this podcast!
Subscribe to CORE IM on any podcast app! Follow us on Facebook @Core IM || Twitter @COREIMpodcast || Instagram @core.im.podcast. Please give any feedback at COREIMpodcast@gmail.com.
Pearl 1: Diagnostic criteria for Contrast-Induced Nephropathy (CIN)
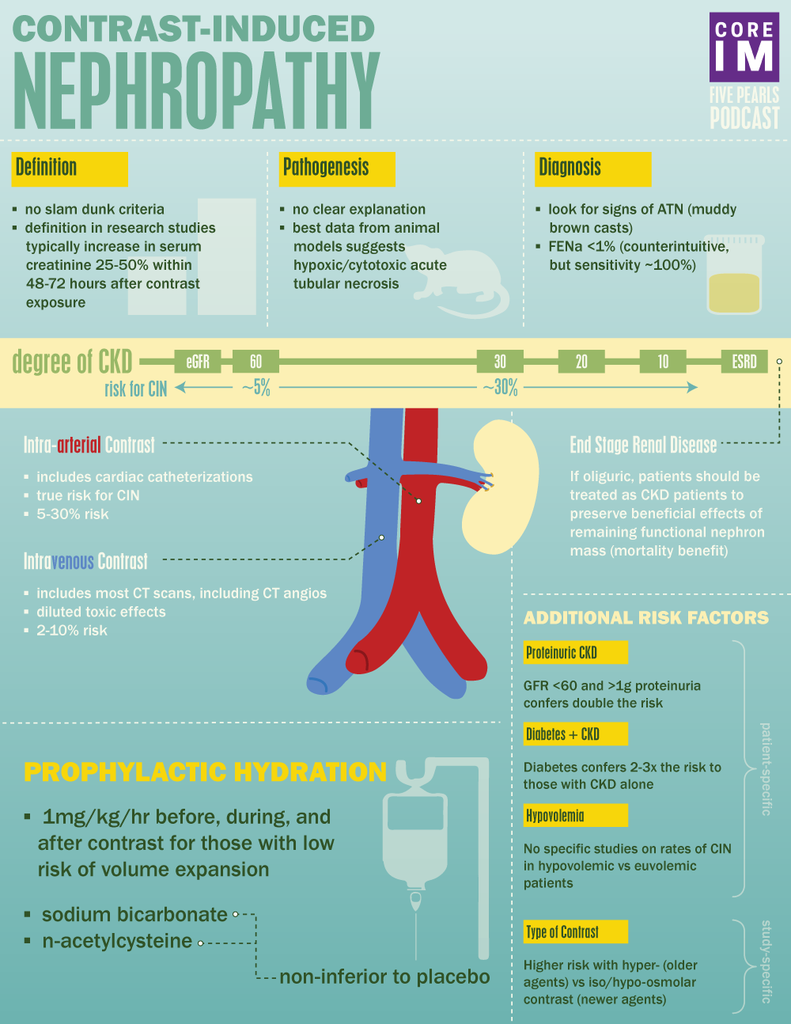
Most research studies define CIN as a relative increase in serum creatinine of anywhere from 25-50% or, an absolute rise in serum creatinine of 0.5 to 1mg/dL within 48-72 hours after exposure to contrast with exclusion of other causes of acute kidney injury.
Other clues are signs of acute tubular necrosis and a fractional excretion of sodium (FeNA) less than 1.
Pearl 2: Intravenous vs Intra-arterial contrast
Most data suggest that CIN is a disease entity almost entirely reserved for patients undergoing intra-arterial contrast loads, and not intra-venous contrast loads.
The incidence of AKI after arterial contrast ranges anywhere from 5-30% depending on the other risk factors present.
The incidence of AKI following intravenous contrast exposure is much lower, in the ballpark of 2-10%
Issues often with studies of arterial contrast:
Retrospective
No control group
Selection Bias
Other variables: showering atherosclerotic emboli to kidneys or volume of contrast used
Issues often with studies of venous contrast:
Also retrospective
Controlled, but poorly
Selection bias
Pearl 3: Risk Factors
* CKD
* Patients with underlying CKD are at increased risk of developing CIN
* Pinpointing the GFR at which the greatest risk occurs is very difficult because most studies lump patients into buckets with wide ranges of GFR
* What we do know:
* In patients undergoing studies with arterial contrast:
* ~ 5% of patients with GFR 30-60 develop CIN
* ~ 30% of patients with GFR <30 develop CIN
* Proteinuria
* GFR < 60 plus at least 1 g of proteinuria develop CIN at almost double the rate of patients with GFR <60 alone
* Diabetes:
* Patients with diabetes coupled with CKD demonstrated almost triple the rate of CIN compared to patients with CKD alone
* Hypovolemia:
* Given difficulty measuring volume status by exam or labs, there are no known randomized trials looking at rates of CIN in those hypovolemic vs. euvolemic
* But given data with prophylactic hydration, low effect arterial blood volume and hypoperfusion to the kidneys are thought to constitute elevated risk.
* High Osmolality Contrast
* Older contrast agents are hyper-osmolar compared to serum and associated with much higher rates of CIN
* Newer contrast agents are either iso-osmolar or hypo-osmolar and associated with rates...
{kind=link}
* Are there diagnostic criteria for contrast-induced nephropathy (CIN)? (2:11 )
* Is there a difference between exposure to intra-arterial versus intra-venous contrast in terms of risk of CIN? (6:28 )
* What are the biggest risk factors for CIN? (14:48 )
* What preventive measures have been shown to best reduce the risk of CIN? (19:41 )
* Can ESRD patients on hemodialysis still suffer from CIN? (23:32 )
* Recap (25:49 )
A special thank you to Dr. Josh Farkas for peer-reviewing this podcast!
Subscribe to CORE IM on any podcast app! Follow us on Facebook @Core IM || Twitter @COREIMpodcast || Instagram @core.im.podcast. Please give any feedback at COREIMpodcast@gmail.com.
Pearl 1: Diagnostic criteria for Contrast-Induced Nephropathy (CIN)
Most research studies define CIN as a relative increase in serum creatinine of anywhere from 25-50% or, an absolute rise in serum creatinine of 0.5 to 1mg/dL within 48-72 hours after exposure to contrast with exclusion of other causes of acute kidney injury.
Other clues are signs of acute tubular necrosis and a fractional excretion of sodium (FeNA) less than 1.
Pearl 2: Intravenous vs Intra-arterial contrast
Most data suggest that CIN is a disease entity almost entirely reserved for patients undergoing intra-arterial contrast loads, and not intra-venous contrast loads.
The incidence of AKI after arterial contrast ranges anywhere from 5-30% depending on the other risk factors present.
The incidence of AKI following intravenous contrast exposure is much lower, in the ballpark of 2-10%
Issues often with studies of arterial contrast:
Retrospective
No control group
Selection Bias
Other variables: showering atherosclerotic emboli to kidneys or volume of contrast used
Issues often with studies of venous contrast:
Also retrospective
Controlled, but poorly
Selection bias
Pearl 3: Risk Factors
* CKD
* Patients with underlying CKD are at increased risk of developing CIN
* Pinpointing the GFR at which the greatest risk occurs is very difficult because most studies lump patients into buckets with wide ranges of GFR
* What we do know:
* In patients undergoing studies with arterial contrast:
* ~ 5% of patients with GFR 30-60 develop CIN
* ~ 30% of patients with GFR <30 develop CIN
* Proteinuria
* GFR < 60 plus at least 1 g of proteinuria develop CIN at almost double the rate of patients with GFR <60 alone
* Diabetes:
* Patients with diabetes coupled with CKD demonstrated almost triple the rate of CIN compared to patients with CKD alone
* Hypovolemia:
* Given difficulty measuring volume status by exam or labs, there are no known randomized trials looking at rates of CIN in those hypovolemic vs. euvolemic
* But given data with prophylactic hydration, low effect arterial blood volume and hypoperfusion to the kidneys are thought to constitute elevated risk.
* High Osmolality Contrast
* Older contrast agents are hyper-osmolar compared to serum and associated with much higher rates of CIN
* Newer contrast agents are either iso-osmolar or hypo-osmolar and associated with rates...

Comments
In Channel

Download from Google Play

Download from App Store
 United States
United States00:00
00:00
x

