


Core IM: 5 Pearls on Troponin
Update: 2019-01-02
Description
By David Rhee MD, Greg Katz MD, Marty Fried MD, Shreya P. Trivedi MD || Illustration by Michael Natter MD || Audio Editing by Harit Shah. Quiz yourself on the 5 Pearls we will be covering:
* What aspects of the history are concerning in a patient with a positive troponin? (4:00 )
* What is the difference between the TIMI, GRACE, and HEART scores, and how should we use them in the evaluation of a patient with an elevated serum troponin? (8:42 )
* Â How does the change in troponin over time help with diagnosis, and what should we consider in a patient with uptrending troponins but an unremarkable EKG? (14:48 )
*  What can a “negative but detectable†troponin tell you about any patient, not just those with suspected ACS? (21:31 )
* Pearls Recap (25:26 )
* Throwback – what are the first-line medications for alcohol use disorder? (28:36 )
Subscribe to CORE IM on any podcast app! Follow us on Facebook @Core IM || Twitter @COREIMpodcast || Instagram @core.im.podcast. Please give any feedback at COREIMpodcast@gmail.com.
Show Notes
Pearl 1: The Value of the Story
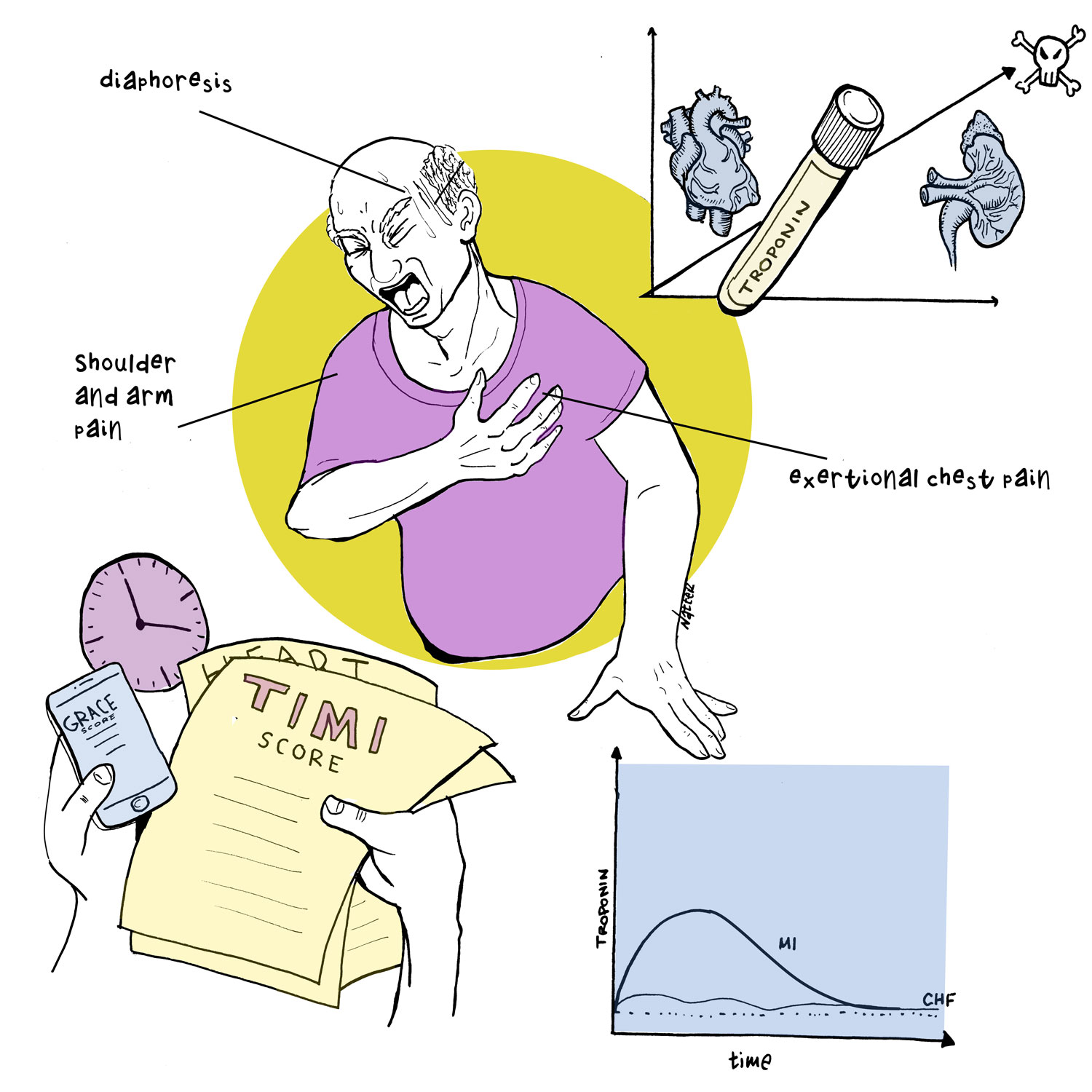
While sensitive and specific to myocyte injury, the troponin is a piece of the clinical picture. Drill down into the HPI and risk factors to determine if this could be ACS.
According to a paper in JAMA 2005, the history of chest pain radiating to the right arm/shoulder had the highest likelihood ratio for a myocardial infarction (LR 4.7), followed by radiation to bilateral arms and shoulders (LR 4.1). However, none of these elements alone or combination of elements in the history can reliably help us rule in or rule out ACS or AMI.
Pearl 2: Risk Stratifying Tools
While there are various tools for risk-stratification, they should serve as adjuncts to your clinical impression and promote thoroughness as a structured checklist.
The TIMI is the most historically validated for percent risk at 14 days of major adverse cardiac event.
The GRACE score accounts for the physical exam and is most useful in those with heart failure or shock.
The HEART score is most often used in the ED for undifferentiated chest pain as a tool to rule out ACS in low risk patients.
Pearl 3: Trending Troponins
Low risk patients in ED (TIMI 0-1) can be ruled out for ACS with 2 negative troponins over 2 hours.
Concerning troponins can be repeated as often as every 2-3 hours. Â
When assessing the acuity of injury, think about troponin trends in terms of changes in log units (i.e. 0.05 to 0.07 vs 0.05 to 5).
If suspicious for ACS but no ST changes on EKG, try posterior and right-sided EKG leads!
The decision to trend troponins to peak is a case-by-case decision.
Pearl 4: Prognostication
Regardless of the primary diagnosis, having elevated troponins in serum is abnormal and predicts worse outcomes in all patients.
Having elevated troponins in patients with ESRD may not indicate ACS, but is still abnormal. It is likely due to the milieu of ESRD inflicting chronic microinjury to the myocardium.
Pearl 5: Throwback to Alcohol Use Disorder
One study found that less than 9% of patients who needed treatment for AUD received a single prescription.
First Line Agents: Naltrexone (1x/day dosing, cannot have cirrhosis or potential use of opioids in the future) and Acamprosate (3x/day dosing).
Transcript
{kind=link}
* What aspects of the history are concerning in a patient with a positive troponin? (4:00 )
* What is the difference between the TIMI, GRACE, and HEART scores, and how should we use them in the evaluation of a patient with an elevated serum troponin? (8:42 )
* Â How does the change in troponin over time help with diagnosis, and what should we consider in a patient with uptrending troponins but an unremarkable EKG? (14:48 )
*  What can a “negative but detectable†troponin tell you about any patient, not just those with suspected ACS? (21:31 )
* Pearls Recap (25:26 )
* Throwback – what are the first-line medications for alcohol use disorder? (28:36 )
Subscribe to CORE IM on any podcast app! Follow us on Facebook @Core IM || Twitter @COREIMpodcast || Instagram @core.im.podcast. Please give any feedback at COREIMpodcast@gmail.com.
Show Notes
Pearl 1: The Value of the Story
While sensitive and specific to myocyte injury, the troponin is a piece of the clinical picture. Drill down into the HPI and risk factors to determine if this could be ACS.
According to a paper in JAMA 2005, the history of chest pain radiating to the right arm/shoulder had the highest likelihood ratio for a myocardial infarction (LR 4.7), followed by radiation to bilateral arms and shoulders (LR 4.1). However, none of these elements alone or combination of elements in the history can reliably help us rule in or rule out ACS or AMI.
Pearl 2: Risk Stratifying Tools
While there are various tools for risk-stratification, they should serve as adjuncts to your clinical impression and promote thoroughness as a structured checklist.
The TIMI is the most historically validated for percent risk at 14 days of major adverse cardiac event.
The GRACE score accounts for the physical exam and is most useful in those with heart failure or shock.
The HEART score is most often used in the ED for undifferentiated chest pain as a tool to rule out ACS in low risk patients.
Pearl 3: Trending Troponins
Low risk patients in ED (TIMI 0-1) can be ruled out for ACS with 2 negative troponins over 2 hours.
Concerning troponins can be repeated as often as every 2-3 hours. Â
When assessing the acuity of injury, think about troponin trends in terms of changes in log units (i.e. 0.05 to 0.07 vs 0.05 to 5).
If suspicious for ACS but no ST changes on EKG, try posterior and right-sided EKG leads!
The decision to trend troponins to peak is a case-by-case decision.
Pearl 4: Prognostication
Regardless of the primary diagnosis, having elevated troponins in serum is abnormal and predicts worse outcomes in all patients.
Having elevated troponins in patients with ESRD may not indicate ACS, but is still abnormal. It is likely due to the milieu of ESRD inflicting chronic microinjury to the myocardium.
Pearl 5: Throwback to Alcohol Use Disorder
One study found that less than 9% of patients who needed treatment for AUD received a single prescription.
First Line Agents: Naltrexone (1x/day dosing, cannot have cirrhosis or potential use of opioids in the future) and Acamprosate (3x/day dosing).
Transcript

Comments
In Channel

Download from Google Play

Download from App Store
 United States
United States00:00
00:00
x

