



Episode 181.0: Subarachnoid Hemorrhage
 6
6Description
We discuss EM presentation, diagnosis, and management of subarachnoid hemorrhage.
Hosts:
Mark Iscoe, MD
Brian Gilberti, MD
Bree Tse, MD
Download
One Comment
Tags: Critical Care, Neurology, Subarachnoid Hemorrhage
Show Notes
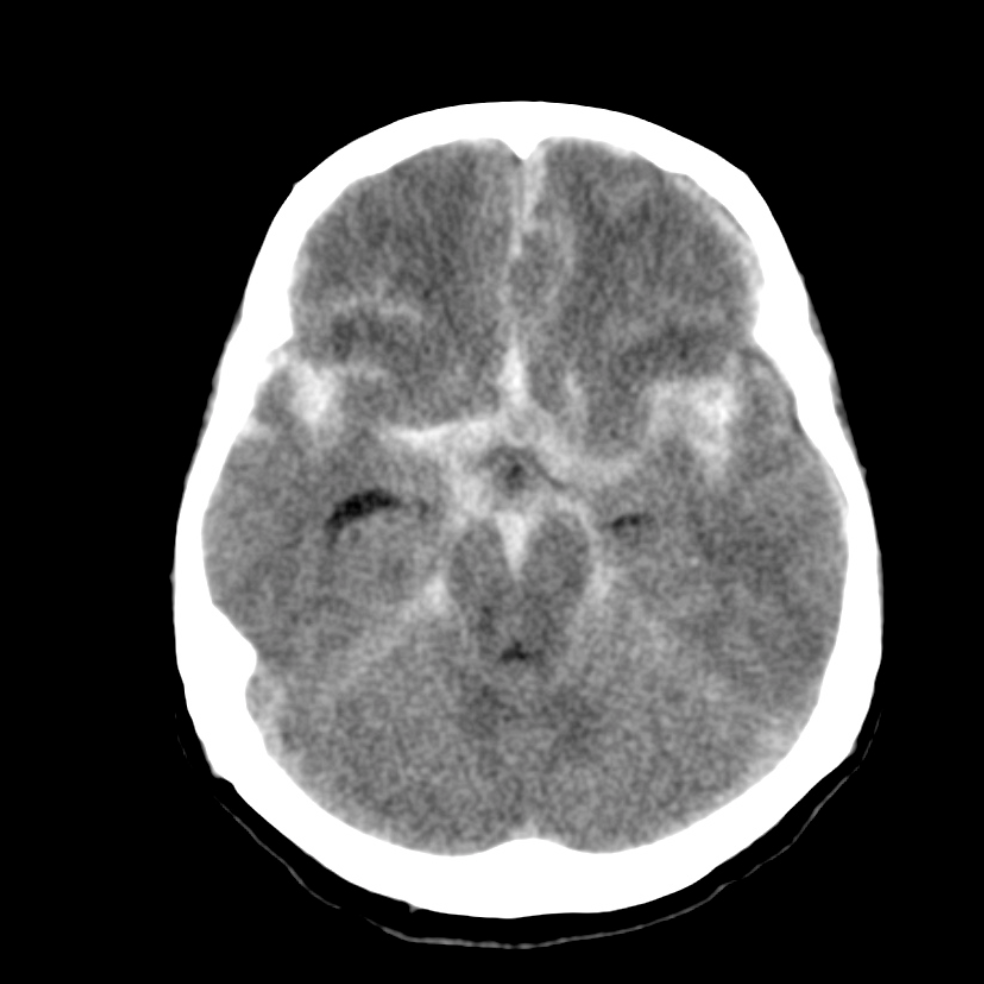
Non-contrast head CT showing SAH (Case courtesy of Dr. David Cuete, Radiopaedia.org, rID: 22770)
Hunt-Hess grade and mortality (from Lantigua et al. 2015.)
| Hunt-Hess grade | Mortality (%) |
| 1. Mild Headache | 3.5 |
| 2. Severe headache or cranial nerve deficit | 3.2 |
| 3. Confusion, lethargy, or lateralized weakness | 9.4 |
| 4. Stupor | 23.6 |
| 5. Coma | 70.5 |
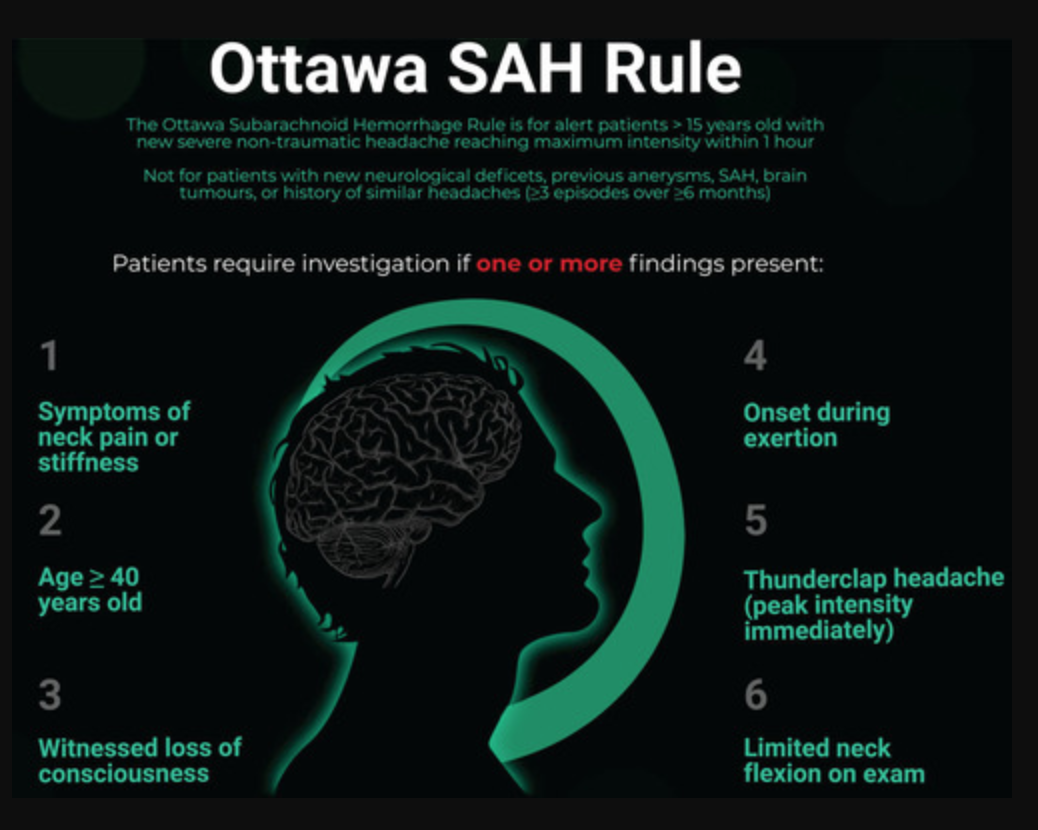
Ottawa Subarachnoid Hemorrhage Rule, and appropriate population for rule application (from Perry et al. 2017)
Apply to patients who are:
- Alert
- ≥ 15 years old
- Have new, severe, atraumatic headache that reached maximum intensity within 1 hour of osnet
Do not apply to patients who have:
- New neurologic deficits
- Previous diagnosis of intracranial aneurysm, SAH, or brain tumor
- History of similar headaches (≥ 3 episodes over ≥ 6 months)
SAH cannot be ruled out if the patient meets any of the following criteria:
- Age ≥ 40
- Symptom of neck pain or stiffness
- Witnessed loss of consciousness
- Onset during exertion
- “Thunderclap headache” (defined as instantly peaking pain)
- Limited neck flexion on examination (defined as inability to touch chin to chest or raise head 3 cm off the bed if supine)
___________________________
Special Thanks To:
- Dr. Mark Iscoe, MD (Ronald O. Perelman Department of Emergency Medicine at NYU Langone Health, NYC Health + Hospitals/ Bellevue)
___________________________
References:
Bellolio MF, Hess EP, Gilani WI, et al. External validation of the Ottawa subarachnoid hemorrhage clinical decision rule in patients with acute headache. Am J Emerg Med. 2015;33(2):244-9.
Carstairs SD, Tanen DA, Duncan TD, et al. Computed tomographic angiography for the evaluation of aneurysmal subarachnoid hemorrhage. Acad Emerg Med. 2006;13(5):486-492.
Connolly ES, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012;43(6):1711-1737.
Czuczman AD, Thomas LE, Boulanger AB, et al. Interpreting red blood cells in lumbar puncture: distinguishing true subarachnoid hemorrhage from traumatic tap. Acad Emerg Med. 2013;20(3):247-256.
Dugas C, Jamal Z, Bollu PC. Xanthochromia. [Updated 2020 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526048/
Goldstein JN, Camargo CA, Pelletier AJ, Edlow JA. Headache in United States emergency departments: demographics, work-up and frequency of pathological diagnoses. Cephalalgia. 2006;26(6):684-90.
Kumar A, Niknam K, Lumba-brown A, et al. Practice Variation in the Diagnosis of Aneurysmal Subarachnoid Hemorrhage: A Survey of US and Canadian Emergency Medicine Physicians. Neurocrit Care. 2019.
Lantigua H, Ortega-Gutierrez S, Schmidt JM, et al. Subarachnoid hemorrhage: who dies, and why? Crit Care. 2015;19:30 9.
Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. 2017;389(10069):655-666.
Mayer PL, Awad IA, Todor R, et al. Misdiagnosis of symptomatic cerebral aneurysm. Prevalence and correlation with outcome at four institutions. Stroke. 1996;27(9):1558-63.
Meurer WJ, Walsh






 United States
United States
